Bispecific therapeutics are about to make a big comeback
Abbvie just announced that they are willing to pay $750M upfront to Genmab to partner on their bispecific therapeutic pipeline, with $3.15B in biobucks milestones if the products are successful. That's a lot of moola. It's probably worth it.
It shouldn't come as a surprise that Abbvie is a believer in bispecific therapeutics. After all, they've been investing heavily in their BiTE immuno-oncology platform with 9 publicly announced therapeutics in the pipeline. They claim that bispecifics are the CAR-T killer, but is it?
TL;DR
If you get the chance, buy into a company doing bispecific cancer therapeutics. CAR-T therapies have a $20B market cap but are limited by manufacturing issues. This is an off-the-shelf solution that could very easily beat it out.
It's like the world's smallest duct tape
Bispecific therapeutics work by grabbing a immune T cell (usually, more later) and a cancer cell. The T cell target is the CD3 receptor - the essential receptor which turns T cells "on" when they bind a target cell. The other target is anything on the tumor.

Obviously specificity matters here. Cancer cells are basically normal cells that have gone haywire, which means most of your potential targets are also expressed on your normal cells. If you chose the wrong one, you risk directing T cells towards the normal cells, to catastrophic results. This is the same risk for CAR-T cell therapies, which led an early leader Juno to pull their candidates after killing multiple patients from a runaway response.
And how does that work?
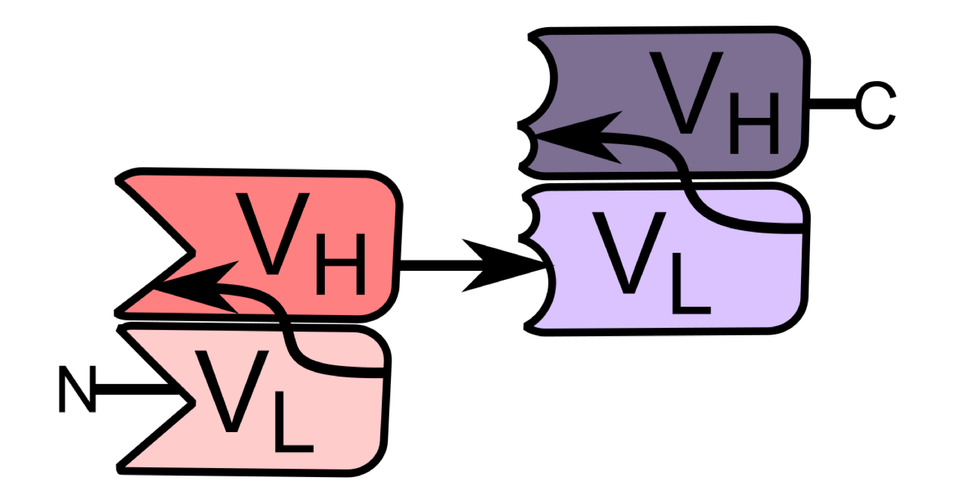
Bispecific therapeutics are not creatively named. Your standard targeted antibody therapy attacks a single target, but an antibody has two binding sites. It's actually expressed (made) as four different protein pieces. The two long ones in the middle and the two matching shorter pieces, here helpfully color coded.
If you swap out one half of this with the pieces of another antibody, you end up with an antibody that binds two different targets - in this case one on the T cell and one on the tumor cell. You could also take all the binding pieces at the end and express them as one single protein that does, functionally, a similar thing. This is Abbvie's pet technology, the so-called BiTE.

{kind=link}
What this does is engage the T cell, the CD3 receptor as mentioned, and create what is known as an immune synapse. It activates the T cell to kill the tumor cell, but only those cells expressing the target of interest.
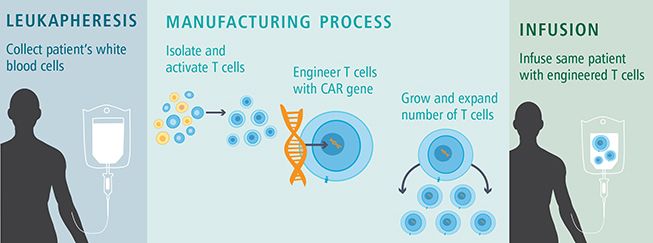
Compare this to CAR-T therapy, which aims to accomplish something very similar. CAR-T cell therapy (chimeric antigen receptor T cell) is a genetically engineered T cell with a special receptor genetically inserted to bind a tumor target. Essentially, it shortcuts the process of your body having to figure out the right targets to destroy tumor cells, which can look very similar to normal cells and be difficult to target. The inside of the CAR-T construct is a potent "KILL" signal that is much stronger than the natural T cell receptor.
Right now, CAR-T has a $20B market cap, driven largely by the fact that it can lead to a long-term and durable cure in advanced hematological (blood) cancers such as B cell lymphoma. And this has led to a veritable gold rush of deals.
The problem with CAR-T is you have to re-make it for every single patient. The patient's T cells are collected, purified, genetically modified, and returned. The process takes weeks, is expensive, and depends on the patient having enough healthy T cells left (not always the case). And did I mention expensive? That's how Kite justified a $373k price tag per patient.
Why did we waste all this time with cell therapies if this is so great?
The short answer is we didn't. Blincyto is approved for use in acute lymphoblastomic leukemia (ALL), a B-cell cancer. But the early versions of bispecifics seemed to only work in hematological (blood) cancers, where CAR-T therapy has proven exceptionally potent. Even if it's long, expensive, and hella dangerous, most people would opt for the higher cure rate.
But CAR-T therapy has stalled out trying to attack solid tumors. The cells just don't seem to penetrate. Further, even the "off the shelf" next gen therapeutics (which would use generic donor cells) are expensive to manufacture, store, and use. Careful monitoring is required post treatment to ensure the cells don't go haywire and start attacking everything, something known as a cytokine storm. Patients are tied to the hospital. Compare this to the promise of an off-the-shelf antibody-like solution, where treatment could be a 15 minute visit every 3 weeks.
Enter Abbvie, and the BiTE platform. Early versions of bispecific therapeutics also have had trouble penetrating solid tumors. Antibodies are big, relatively speaking, and just can't get into the tight, poorly vascularized middle of the tumor. The BiTE configuration is a slimmed-down antibody, using just the sticking binding sites and a short bit of linker protein. This has the added benefit of vastly simplifying manufacturing, a mundane but essential consideration behind the scientific hype. A quick glance at the Abbvie BiTE pipeline reveals a few hematological tumor targets (BCMA, CD19), but a heavy lean into solid tumor targets (EGFR, MUC17). These are classic "targeted therapy" targets, which means we know they work, but with a brand new immunotherapy dressing.
What are the risks
The main problem with this new strategy is half life. Antibodies are made to exist within your blood stream for weeks, even months, which is why antibody-based therapeutics have a really nice dosing schedule. But the BiTE platform is small, and has a short half life of only a few hours. That means it requires much more frequent dosing (daily instead of weekly) but unlike a small molecule drug packaged into a pill it has to be given via injection. Sort of a worst of both worlds thing.
Abbvie has extended their platform to include a "Half Life Extended" version which brings back the Fc domain of the antibody. The Fc domain is the big tail on the antibody and is essential to long-term persistence of the therapeutic. Interestingly, it can also be functional - NK cells recognize this to figure out what cells to kill even though they themselves do not have a "learning" function. The Amgen patent is unclear on whether they envisioned this as a functional part of their therapeutics.
Further, the cell therapy field hasn't shown any signs of slowing. Be it an allogenic CAR-T strategy (Allogene), specifically-expanded CAR-T cells (Allovir), or CAR-NK cells (MD Anderson, Takeda), researchers are promoting multiple strategies that will at least enable more rapid patient therapies. Whether these strategies overcome the limited efficacy in solid tumors seen in early generations, though, remains to be seen.
But wait there's more
We haven't even gotten to some of the new fun tech out there. Dragonfly Therapeutics is positioning itself as an NK cell-targeted therapeutic (the other major anti-tumor immune cell), but it's essentially a bispecific therapeutic class binding a special receptor expressed on both NK and CD8 T cells. We'll have to get that next time.
Disclaimer
None of the above should be construed as investment advice. I'm just a PhD digging through the biology behind biotechs and not a certified investment analyst. I am also a shareholder in Courier Therapeutics, a startup in the cancer immunotherapy space. Talk to your financial advisor before buying and selling equities.